Facial Contouring Revision Surgery: A Case Study on Correcting Mid-Face Fullness
- Dr. Park

- Jun 19, 2025
- 4 min read
Patients undergo facial contouring surgery with the expectation of achieving a slimmer, more refined facial structure. However, in some cases, patients report that despite significant bone reduction in the mandible and zygoma, their mid-face region appears fuller or wider post-operatively.
This posting presents a clinical case study detailing the diagnosis and successful management of this specific concern through revision facial contouring surgery. We will provide an objective analysis based on clinical data, including 3D CT scans and body composition analysis, to explain the cause of this phenomenon and the effectiveness of a comprehensive surgical solution.
Analysis of Post-Operative Changes: The Cause of Mid-Face Fullness
The patient had previously undergone a primary facial contouring procedure with the following details:

Primary Surgery Summary:
T-Osteotomy Genioplasty: 3mm vertical lengthening, 4mm width reduction.
Mandible Angle Reduction: Resection of the mandibular angle, cortical osteotomy, and masseter muscle reduction.
Zygoma Reduction (Malarplasty): 3mm resection of the 45-degree malar region, 6mm inward repositioning of the zygomatic arch.
In the year following the surgery, the patient's body composition changed, showing a 2.7 kg increase in weight, a 10.2% increase in body fat percentage, and a 2.1 kg decrease in muscle mass.
A common misconception is that weight gain after facial contouring will cause soft tissue to sag below the resected bone. However, the clinical reality is often different. When the underlying skeletal framework is reduced, any subsequent increase in soft tissue volume (fat and muscle) tends to redistribute. Instead of sagging, this volume often concentrates in the adjacent mid-face area, influenced by the repositioning of the masseter muscle and buccal fat pad.

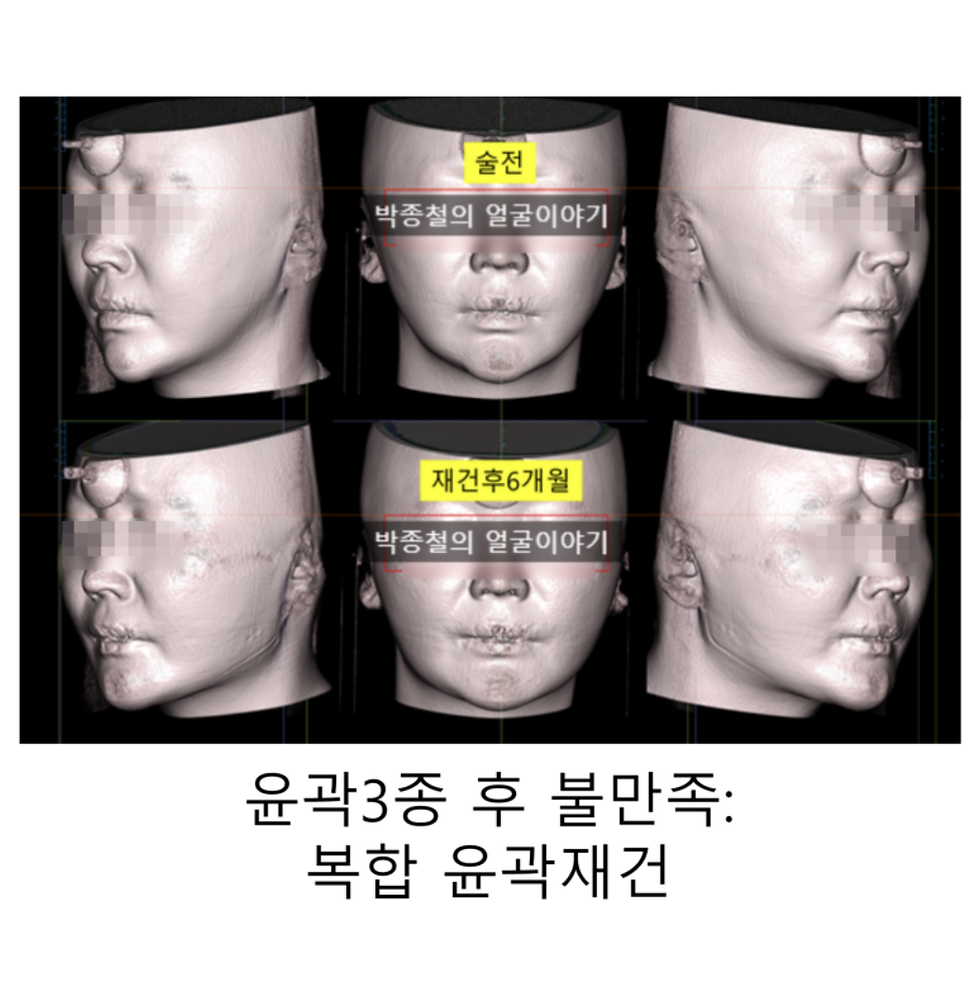
This was confirmed by superimposing the patient's pre-operative and 1-year post-operative 3D soft tissue images. The analysis clearly showed that the post-operative soft tissue volume (in cyan or teal color) had accumulated in the mid-face region. This anatomical shift was the primary reason the patient's face appeared fuller despite the bone reduction.

Surgical Planning for Revision Facial Contouring
The patient's goals for the revision were to achieve additional reduction of the 45-degree zygoma and to further lengthen the chin to improve overall facial harmony. To address these goals and effectively reduce the concentrated mid-face volume, a comprehensive revision plan was established:
Revision Zygoma Reduction: Additional resection of the 45-degree zygoma (2mm on the right, 1mm on the left) to reduce anterior projection.
Additional Mandibular Cortical Osteotomy: To further reduce the overall width of the lower face from a frontal view, targeting the outer layer (cortex) of the mandible.
Buccal Fat Removal: Direct removal of the buccal fat pad, a key contributor to mid-cheek volume. (Volume removed: 4.2cc from the right, 3.8cc from the left).
Revision T-Osteotomy Genioplasty: 2mm of additional vertical lengthening and 2mm of advancement to enhance the chin's projection and improve the vertical balance of the face.
Mini-Facelift: Performed concurrently to address any potential soft tissue laxity after volume reduction and to ensure a tight, refined final contour.
Objective Results Confirmed by Clinical Data
Substantial Reduction in Mid-Face Volume A cross-sectional CT scan taken 6 months after the revision surgery confirms a significant reduction in mid-face volume. To visualize this change, the pre-revision soft tissue contour (yellow curve) was superimposed onto the post-revision CT image. The image clearly demonstrates that the patient's new facial contour lies well inside the previous yellow line, indicating a definitive reduction achieved through the cortical osteotomy and buccal fat removal. The patient also undertook a weight loss regimen alongside the surgery, resulting in a 5 kg decrease in body weight and a 2.6% decrease in body fat, which contributed to the favorable outcome.



2. Skeletal and Soft Tissue Changes Post-operative CT analysis confirmed that the chin was successfully lengthened by a measured 3.55mm. This structural modification plays a crucial role in creating a more balanced vertical proportion, drawing the aesthetic focus away from the width of the mid-face.


Over the total 1.5-year period encompassing both surgeries, the patient's final body composition showed a net weight loss of 2.3 kg, a net muscle loss of 5.0 kg, and a net body fat increase of 7.6%. Despite these complex metabolic changes, the patient's facial appearance was markedly slimmer and more defined after the revision surgery. This underscores the impact of the structural surgical corrections. The aesthetic improvement was driven primarily by the surgical reduction of bone and fat volume, not just by weight loss.

Conclusion: A Comprehensive Approach to Successful Revision Facial Contouring
The phenomenon of increased mid-face fullness after facial contouring is a multifactorial issue resulting from the interplay between skeletal reduction, soft tissue redistribution, and changes in body composition.
Therefore, an effective solution requires more than a simple, isolated procedure like liposuction. As this case study demonstrates, a successful outcome is achieved through a comprehensive and strategic surgical plan. The combination of mandibular cortical osteotomy to reduce facial width, buccal fat removal to target specific volume, genioplasty to optimize facial proportions, and adjunctive procedures like a mini-facelift to tighten the soft tissue envelope can effectively resolve the issue.
Patients experiencing unsatisfactory results from a primary procedure should seek consultation with an experienced Oral and Maxillofacial Surgeon for an accurate diagnosis and a tailored surgical plan to achieve their desired aesthetic goals.



Comments