Preventing Asymmetry Relapse After Double Jaw Surgery: The Key is Solving 'Bone Defects'
- Dr. Park

- Oct 1, 2025
- 4 min read
Many patients hope to correct facial asymmetry and regain a beautiful, balanced facial harmony through orthognathic surgery (double jaw surgery).
A successful orthognathic surgery must satisfy three core elements:
Proper Surgical Planning: The stage of accurately diagnosing the patient's condition to create a plan that will yield optimal results.
Precise Surgical Execution: The surgeon's technical skill in implementing the sophisticated plan without error.
Long-Term Stability of Results: Ensuring that the surgical outcome remains stable and maintained over time.
Today, I would like to focus on the third element, which is a major concern for many patients: the 'long-term stability of results.' I will explain in depth, with a real patient case study, our efforts to prevent the recurrence of asymmetry after orthognathic surgery.
The Starting Point of Asymmetry Relapse: The 'Bone Defect'
When we create a detailed surgical plan using 3D simulations to correct facial asymmetry, we inevitably identify spaces that are created when the bone is moved to its ideal position. This is known as a 'bone defect' or 'bone gap.' It is an unavoidable aspect of the process of correcting asymmetry.

What happens if the surgery is completed without properly filling and reinforcing this bone defect? Our jawbones must withstand surprisingly strong forces.
Repetitive chewing (masticatory) forces during meals.
Powerful teeth grinding (bruxism) habits during sleep, strong enough to wear down teeth.
This continuous load is applied to the newly positioned jawbone. If the bone defect area has a weak foundation, it may not withstand these forces and can undergo micro-deformations. This can lead to the unfortunate outcome of asymmetry relapse after double jaw surgery.
A Precise Solution to Prevent Relapse: Custom Plates and Bone Grafting
To minimize the possibility of such relapse, I apply a more precise solution utilizing a digital orthognathic system: the combined use of 'patient-specific fixation plates' and 'bone grafting.'

We design and fabricate fixation plates that are optimized for each individual patient, ensuring that the identified bone defect can be filled in a stable manner. This custom plate serves not only to fix the bone but is specially designed to secure the bone graft and provide the necessary space for the grafted bone to heal and integrate properly.

Verifying Long-Term Stability: A Case Study with 5-Month Follow-up CT Scans
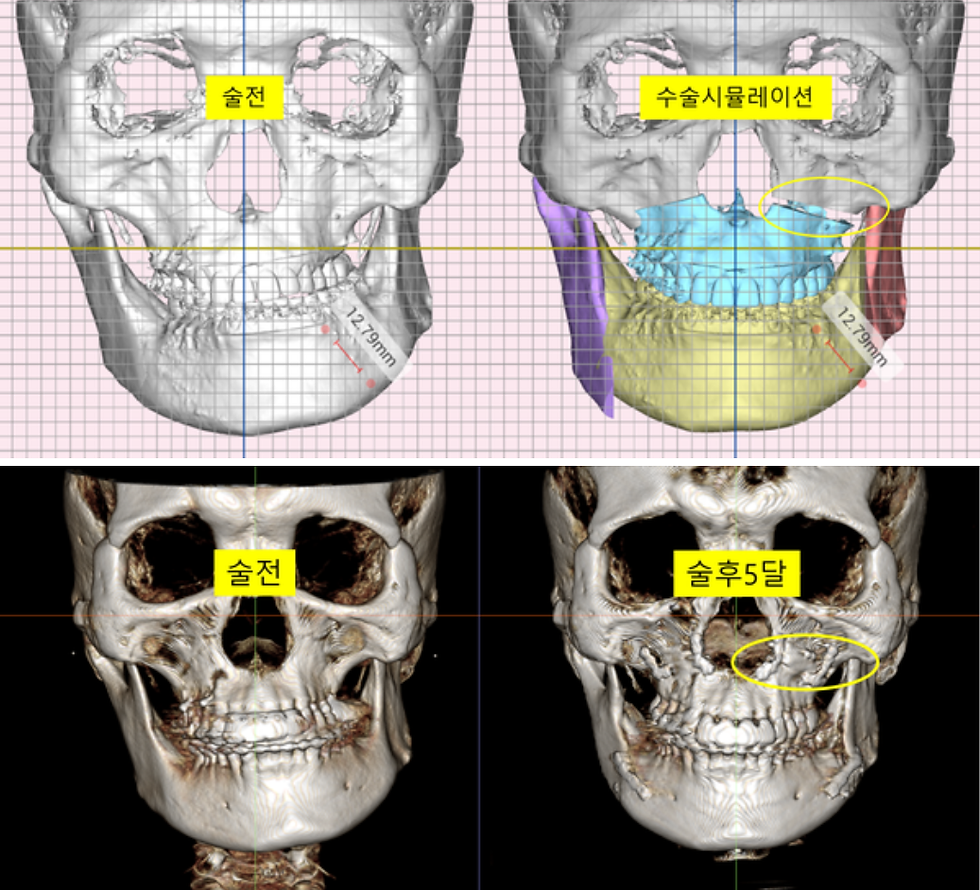
The following are pre-operative and 5-month post-operative 3D CT scans of a patient who underwent asymmetry correction surgery with bone grafting according to the plan described above. We can objectively confirm that the asymmetry was satisfactorily corrected in line with the skeletal midline.
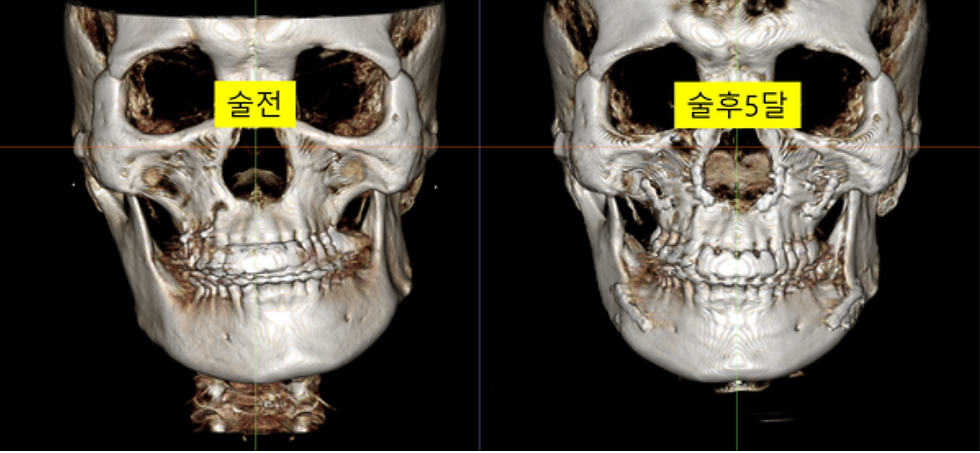
More importantly, let's look at the change in the bone defect area. The bone defect on the left side of the maxilla (upper jaw), which was predicted in the surgical simulation, is now observed on the 5-month post-operative CT scan to be filled and rigidly united with new bone. This signifies that a stable foundation has been successfully established.
The most objective way to check for asymmetry relapse after orthognathic surgery is to compare the immediate post-operative results with those after a certain period. By superimposing the CT scan from 3 days post-op with the scan from 5 months post-op, we observed no clinically significant relapse (recurrence) of asymmetry. This strongly suggests that creating a stable skeletal foundation through bone grafting had a positive impact on the long-term stability of the results.

Conclusion: Sustainable Results are a Collaborative Effort
Achieving a successful surgical outcome that lasts for a long time is not accomplished by the surgeon's efforts alone. The patient's active cooperation, including myofunctional therapy (MFT) and mouth-opening exercises to help the surrounding muscles adapt to the new skeletal structure, is absolutely essential.
However, as demonstrated in this case, a surgeon's role is critical in ensuring a lasting result. By predicting bone defects from the planning stage using a digital orthognathic system and meticulously performing a precise bone graft in that area, we can provide a much more stable skeletal foundation. I believe this is the surgeon's most important responsibility in preventing asymmetry relapse after double jaw surgery.



Comments