SSRO & IVRO: A Comparative Study of Postoperative Skeletal Changes and Condyle Positioning
- Dr. Park

- Jan 26, 2025
- 3 min read
Mandibular orthognathic surgery, a surgical procedure to correct jaw alignment and restore function, often involves two primary techniques: sagittal split ramus osteotomy (SSRO) and intraoral vertical ramus osteotomy (IVRO). This posting will delve into the distinctions between these two procedures, analyze postoperative skeletal changes, and emphasize the significance of personalized treatment approaches.
Surgical Techniques: SSRO vs. IVRO
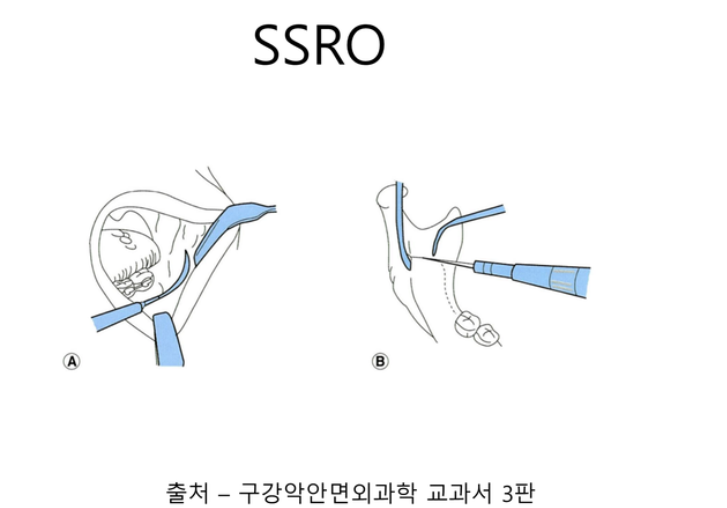
Sagittal Split Ramus Osteotomy (SSRO)
In SSRO, the mandibular ramus is divided along a sagittal plane. This method prioritizes maintaining the condyle's position as close as possible to its preoperative state. The bone fragments are fixed using metal plates, ensuring immediate postoperative stability.
Sagittal Split Ramus Osteotomy (SSRO) 
Sagittal Split Ramus Osteotomy (SSRO)
Intraoral Vertical Ramus Osteotomy (IVRO)
IVRO involves a vertical cut of the mandibular ramus. Unlike SSRO, it does not employ metal plates; instead, postoperative recovery is facilitated by maxillomandibular fixation for approximately two weeks. The condyle's position is adjusted through physical therapy to achieve a functional position.

Intraoral Vertical Ramus Osteotomy (IVRO) 
Intraoral Vertical Ramus Osteotomy (IVRO)
Postoperative Skeletal Changes
SSRO Postoperative Changes
Following SSRO, the condyle's position remains relatively stable. Even if the condyle shifts downward slightly, it typically returns to its original position within 3 to 5 weeks. Excessive rotation or displacement is uncommon. The metal plate fixation contributes to enhanced postoperative skeletal stability.

SSRO Postoperative Changes 
SSRO Postoperative Changes 5 weeks
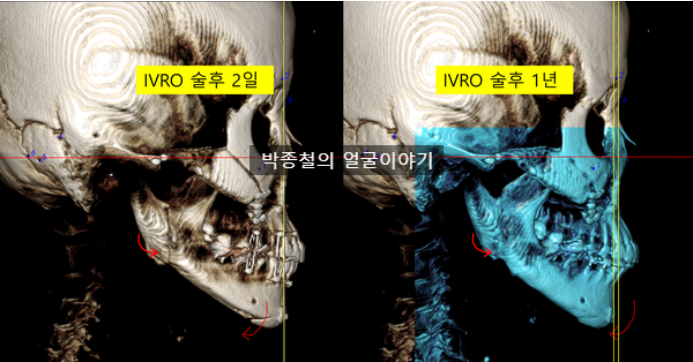
IVRO Postoperative Changes
In IVRO, the condyle tends to shift anteriorly and inferiorly, establishing a new equilibrium within a year. The condyle also rotates counterclockwise, adapting to a position different from its preoperative state. However, there is insufficient evidence to definitively conclude that the condyle's new position in IVRO is more physiologic.

IVRO Postoperative Changes
Considerations on the Physiologic Equilibrium of the Condyle
The term "physiologic equilibrium" in relation to IVRO can be misleading. It might suggest that IVRO guides the condyle to a more physiologically suitable position. However, most orthognathic surgery patients do not experience temporomandibular joint (TMJ) symptoms preoperatively, indicating that their condyle's position is already functionally sound. Therefore, rather than describing the condyle as finding a "physiologic position" in IVRO, it is more accurate to state that it achieves a "functionally stable new position." IVRO involves a process of adaptation where the condyle settles into a new position, leading to skeletal changes. In contrast, SSRO aims to maintain the condyle's position as close as possible to its preoperative state. While both techniques differ in their perspectives on the ideal condyle position, a functionally sound condyle position can be considered a "physiologic equilibrium."
Impact of Condyle Sagging
"Condyle sagging," the downward displacement of the condyle postoperatively, can occur in both SSRO and IVRO but with varying degrees and implications.
SSRO Condyle Sagging: Condyle sagging is less pronounced in SSRO, and even if it occurs, the condyle typically returns to its original position. Although the final stable position may differ slightly from the immediate postoperative position, this difference is generally smaller compared to IVRO.

SSRO Condyle Sagging IVRO Condyle Sagging: In IVRO, sagging and rotation occur as the condyle seeks a functionally stable position. This can result in a final skeletal position that differs from the preoperative plan.
IVRO Condyle Sagging
Condyle sagging can influence postoperative skeletal changes and the longevity of surgical outcomes. Therefore, it is crucial to consider this factor during surgical planning. Even with SSRO, the possibility of the condyle shifting away from its immediate postoperative position within the first month cannot be entirely ruled out.
The Importance of Customized Titanium Plates in Sagittal Split Ramus Osteotomy (SSRO)
Utilizing customized titanium plates in sagittal split ramus osteotomy (SSRO) procedures significantly enhances the precision and predictability of surgical outcomes. By tailoring these plates to each patient's unique anatomical features, surgeons can more accurately position and stabilize the mandibular condyle, minimizing the risk of postoperative complications like condyle sagging.
Conclusion
Both SSRO and IVRO have their unique advantages and disadvantages. The optimal technique should be selected based on the patient's individual condition and treatment goals. SSRO offers greater postoperative condyle position stability and accuracy, while IVRO provides more flexibility in achieving functional stability. However, IVRO carries the risk of compromised long-term results due to condyle sagging and rotation. To ensure optimal patient outcomes, I prefer a personalized approach that primarily involves SSRO with customized metal plates. Precise surgical planning and patient-specific metal plates are essential for achieving the best possible results. By thoroughly evaluating each patient's condition and prioritizing condyle stability, successful surgical outcomes can be consistently achieved.
For more detailed information, please refer to the video below.



Comments